Paracolic Gutter Fluid Ct

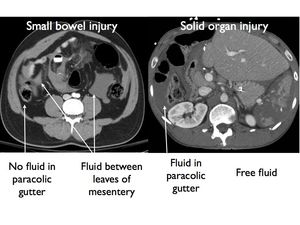
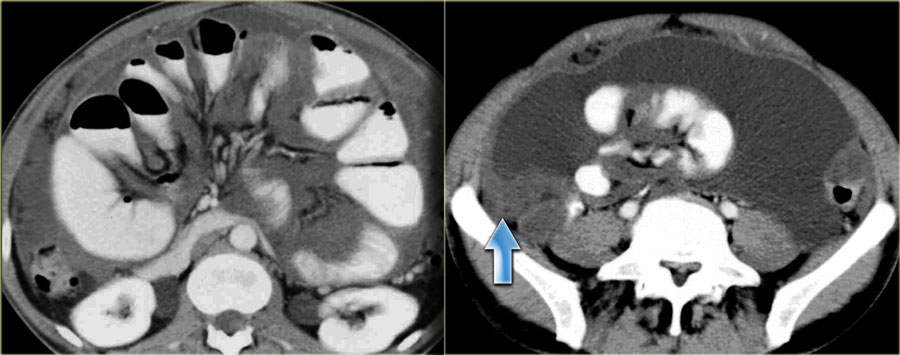
Ct Showing Free Fluid In The Right Paracolic Gutter No Free Air And Download Scientific Diagram
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 133725

Abdominal Computed Tomography Ct Revealed Fluid Accumulation In The Download Scientific Diagram

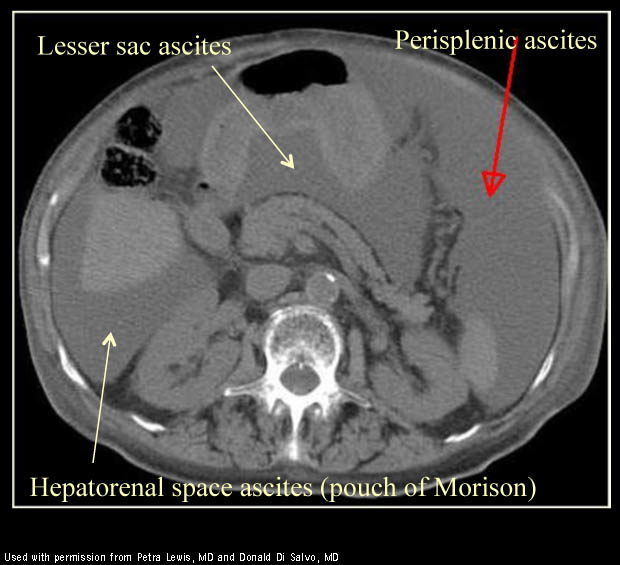
Free Intraperitoneal Fluid Summary Radiology Reference Article Radiopaedia Org
Abdominal Ct An Axial View Demonstrated A Mild Amount Of Fluid In The Download Scientific Diagram

Ct Scan Visualizes A Large Fluid Collection Fc In The Retroperitoneal Download Scientific Diagram

The main paracolic gutter lies lateral to the colon on each side.
Paracolic gutter fluid ct.

Epos
Abdominal Xray Ct Us Radiology Flashcards Memorang
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 127176

Coronal Section Ct Image Demonstrating Fluid Collection Extending Down Download Scientific Diagram
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 117837

Frontal Reformatted Ct Image A Fluid Collection Is Noted In The Left Download Scientific Diagram
Epos
Fitz Hugh Curtis Syndrome Radiology Case Radiopaedia Org
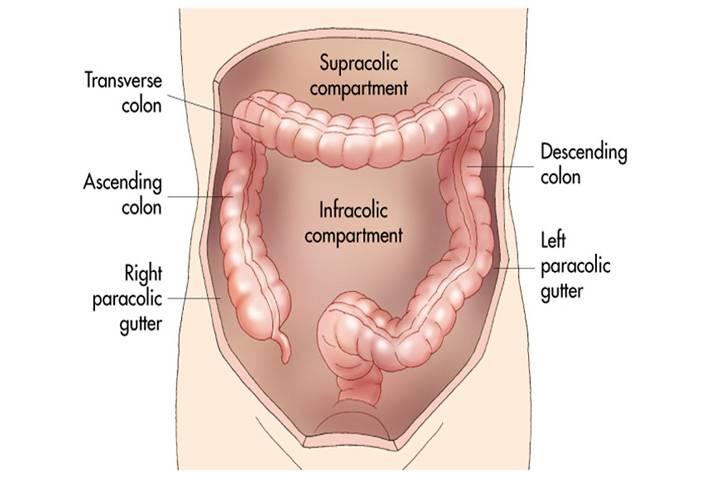
Paracolic Gutter
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 115818
The Radiology Assistant Peritoneal Pathology

Ct Scan Of Abdomen Showing Ruptured Haemangioma With Free Fluid In Download Scientific Diagram

Intra Abdominal Collections Radiology Case Radiopaedia Org
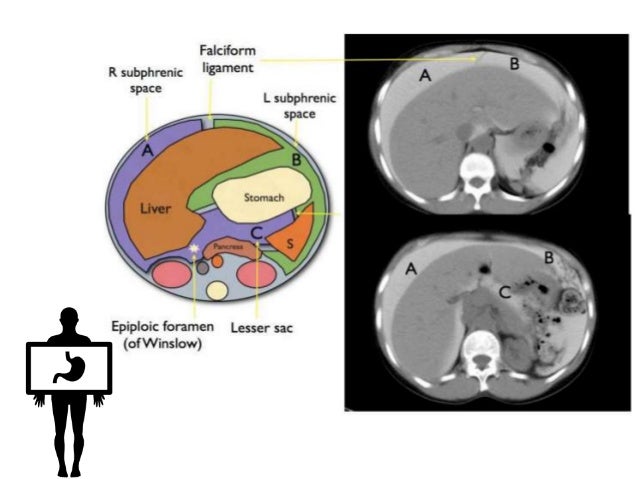
Peritoneum Intraperitoneal Spaces

Subcapsular Haematoma Of The Spleen Complicating Acute Pancreatitis Bmj Case Reports

Ct Abdomen And Pelvis Without Contrast Coronal View Showing Small Download Scientific Diagram

Pancreatic Injury Post Laparoscopic Subtotal Colectomy There Is Pancreatic Fluid Tracking From The Pancreatic Tail Arrows To Th Colectomy Abdomen Pancreatic

Penetrating Stab Injuries To The Anterior Abdomen Use Of Multi Detector Computed Tomography To Predict The Need For Laparotomy
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcshgccvhjwl4fga6xmtvrtmvxwjd3da6xh699xbs0yifrpvajgq Usqp Cau

Small Bowel Ischemia Radiology Case Radiopaedia Org

Figure 1 Toxicity From Intra Abdominal Injection Of Chlorfenapyr
Https Link Springer Com Content Pdf 10 1007 S002619900575 Pdf

Ewing Sarcoma Of The Spine Radiology Case Radiopaedia Org

The Abdominal Wall And Peritoneal Cavity Radiology Key
Source : pinterest.com
